Meet "Zoe," a 13 year old, FS, DSH. She weighs 11.63 lbs; BCS = 6/9. *She had lost 1 pound since last visit (6 months ago).
Presenting Complaint: lethargy and hyporexia x 2-3 days.
Exam Findings:
Temp = 105.3 F
QAR; icteric sclera; increased skin turgor, tacky and mildly icteric mucous membranes.
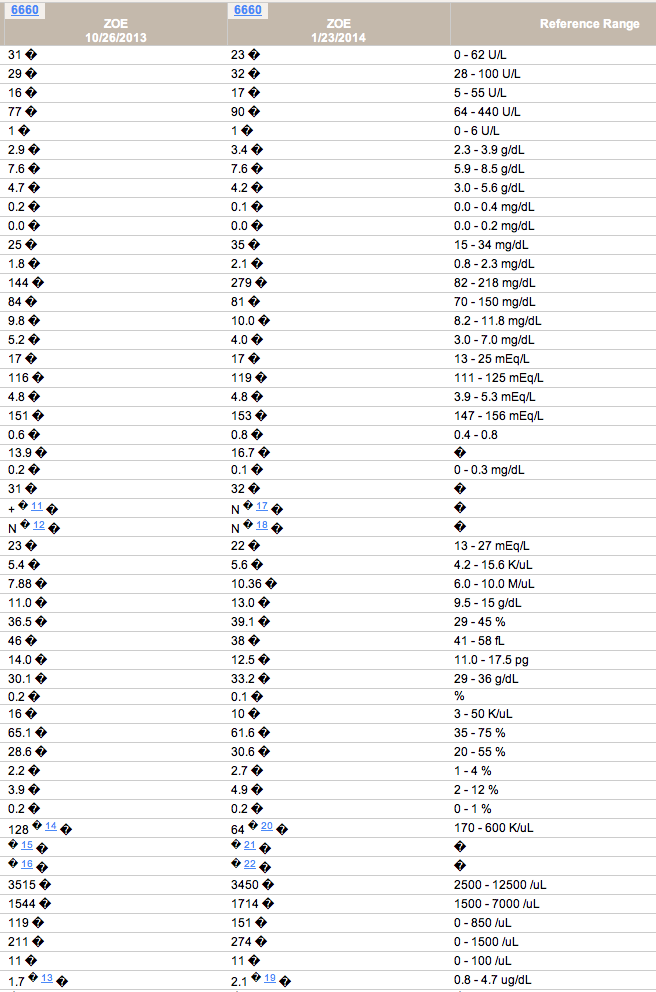
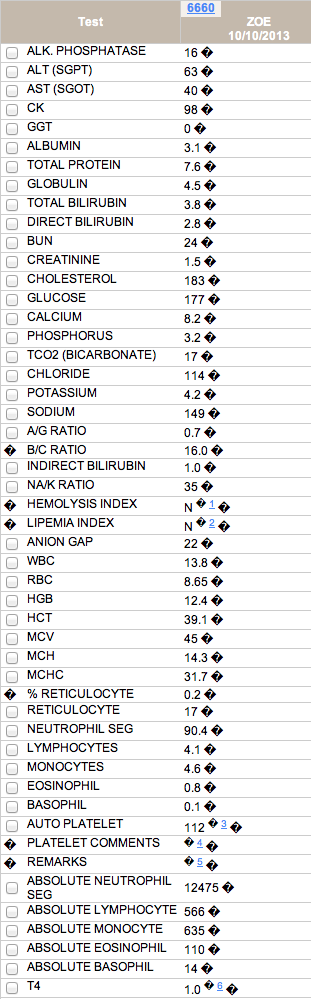
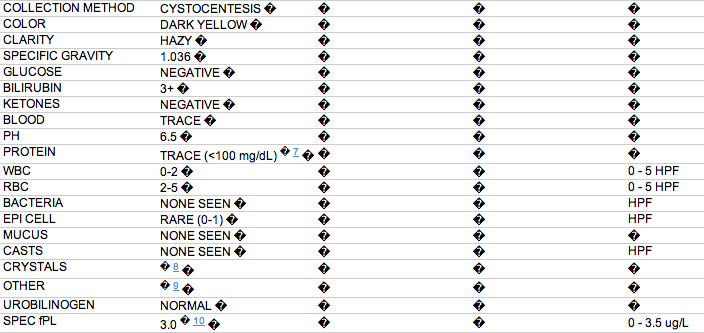
Here are initial blood test and urinalysis results for this patient:

Question: Differentials at this point? Thoughts about how to proceed? Initial Treatment? Next in Diagnostics?


Let's see - how about an FeLV/FIV test? I like to be sure we do this on every sick cat.
Some thoughts (in no particular order):
- When I see total bilirubin getting above 3.0 mg/dL, I think most strongly about hepatobiliary disease rather than other causes of hyperbilirubinemia (and we don't have evidence of hemolysis in this case).
- Any degree of bilirubinuria is significant in cats
- Cats can have liver disease with normal liver enzymes
- Given that her physical examination shows dehydration, I am surprised her urine SG is not higher. What kind of diet is she on? Cats eating only canned food diets can have lower normal urine SG than cats on dry diets.
- her temp of 103.5F is pyrexic, correct? (Fahrenheit challenged Canadian here!). Pyrexia can be from inflammation or infection.
So her problem list:
- hyporexia (2-3 days but probably longer)
- icterus
- pyrexia
- weight loss
- dehydration
I'd like to know what her serum cobalamin level is.
Initial treatment would involve rehydration and I'd give cobalamin (after a sample is drawn to test levels).
Any clues she might be nauseous (lip smacking, turning away from food, etc)? I'd probably assume she is nauseous and give her maropitant or mirtazapine. We can give mirtazapine to patients with liver or kidney disease but it is best to extend the dosing interval (same for maropitant).
I'm surprised that her CK isn't higher as with that amount of weight loss, I would suspect she has been anorectic longer than the owner reported and CK levels tend to increase quite a bit in anorexia/hyporexic cats with weight loss. Most owners feed cats ad lib and so don't tend to notice hyporexia until it is more advanced. CK levels can actually be used to monitor progress in anorexic cats as they tend to decline when adequate nutritional support is provided.
We'll need to estimate her current daily caloric intake and have a plan for nutritional intervention within about 24 hrs, regardless of her underlying disease and ongoing investigations.
Do we know what her fecal score is?
And I think some imaging is in order! Was her abdominal palpation totally normal? Any sign of abdominal pain?
Susan
My handy online Celsius convertor says 105.3 F is 40.7 C. The normal cat body temperature is 37.8- 39.0 C. Here fever is quite significant. All of your observations are spot on, Dr. Little.
What made this case a little more challenging happens to all of us every day - context. While the history included hyporexia of about 2-3 days, what I learned after listening for awhile is that this usually very observant and informed client usually gave me all the information I needed, there were distractions happening. Her husband had recently been diagnosed with a life threatening illness. After we talked for awhile, it became clear that Zoe had been observed less closely than usual and, perhaps, had been not herself for a time. She reminded me of how important it is to allow clients to tell their whole story. Stay tuned...
So, Zoe was hospitalized (she did vomit while in the hospital) and the initial treatment plan was:
- IV Fluids
- Fluoroquinolone to address the fever
- Cerenia
- Vitamin B12
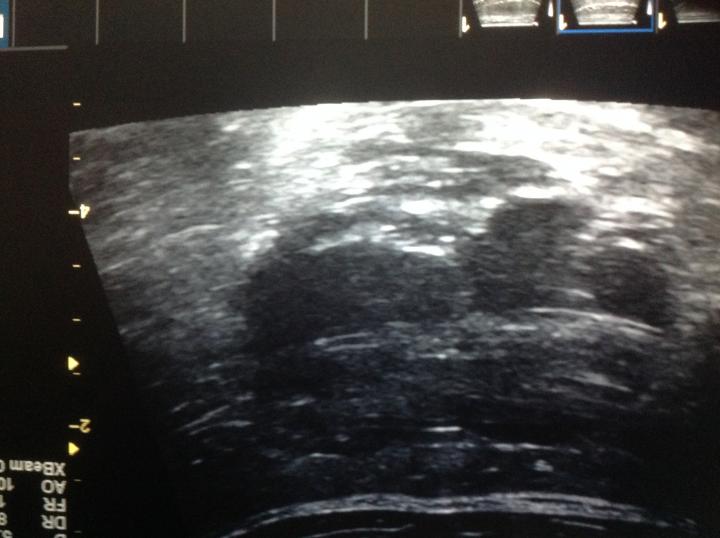
An abdominal ultrasound was performed (image below). The liver parenchyma appeared normal though there was a 4 cm fluid filled structure believed to be compressing and obstructing the gall bladder.
Opinions by a surgeon and ultrasonographer concluded that bile flow was not obstructed.
The owner was informed that surgical exploration may be necessary as well as placement of an esophagostomy tube should she not improve with empirical treatment. Owner agreed.
Zoe was maintained on IV fluids, four quadrant antibiotic therapy and Cerenia for 3 days.
Our working diagnosis was infectious cholangitis.
She continued to improve and began to eat on her own while hospitalized. She was discharged on day 4. Her follow up lab values improved: